
Cross-Examination: An Impossible Choice - 'Seales v Attorney-General'

Lecretia Seales' application to the High Court for declarations stating that her physician was able to assist her, as an individual facing an incurable and intolerable terminal disease, to end her life is the latest in a large number of assisted suicide cases to have come before the common law courts in recent years. Today, Communications Co-Manager Sebastian Hartley provides an in-depth analysis of the sections of Justice Collins' judgment in 'Seales v Attorney-General' relating to Ms Seales' challenging the effect of the Crimes Act in regards to assisted suicide, in which his Honour refused to grant Ms Seales' applications.
Readers are advised that this article contains extensive discussion of suicide. If anybody is contemplating suicide, or has had suicidal thoughts, they are able to seek help through the support services whose contact details are listed at the bottom of the article.
---
To kill one’s self is no crime in New Zealand. Therefore, if an individual who faces the prospect of the gradual loss of bodily function and integrity from the effects of a terminal illness takes their own life, rather than endure the grievous suffering such illnesses can produce, it is no crime for them to do so.
Parliament has made it abundantly clear, however, that anybody assisting such a person to do the same is committing a serious crime. Section 63 of the Crimes Act 1961 provides that an individual cannot give legally effective consent to the intentional infliction of death on themselves.[1] Therefore if any person, including a physician, was to take a positive act to end the life of a terminally ill person, that would be culpable homicide contrary to s 160(2)(a) Crimes Act 1961 as it would be impossible to raise consent to negate the assault.[2] Indeed, since that act would be done with the intention to kill the sufferer, it would almost certainly be murder.[3]
Furthermore, even if no positive act was taken, but the patient was simply provided with the means of ending their own life, that would still be to aid a suicide.[4] In fact, since merely omitting to prevent someone from doing something, where that omission is intended to encourage them do that thing, and does so, it may well also be an offence against s 179 for a person’s loved ones to be present for the end of their life, or even for their not stopping their loved one from ending their life on their own.[5]
Effectively, therefore, these provisions contribute to the creation of a dual standard of death. On the one hand are those who are able to take their own life without potentially implicating their loved ones. On the other hand are those, who will often be individuals suffering, as Lecretia Seales was, from a “grievous and terminal illness that causes enduring suffering that is intolerable to the individual.”[6] These individuals are those who are either physically unable to end their own life, because of the deterioration of their condition, or who are unwilling to take their life alone and in secret to avoid their loved ones being implicated, meaning that they must impose upon their loved ones the burden of finding their body, and being denied a final goodbye.
Ultimately, their choice becomes an impossible one. One course of action is to “suffer through to the bitter end without choice”[7] as their condition continues to deteriorate, possibly beyond the limits of palliative care; which care may cause impairment of cognitive function in severe cases. The other is to take their lives whilst they retain the ability to do so rather than waiting for their illnesses to cause further debilitation.[8] They are forced to either live on whilst the circumstances of their existence are intolerable, or to end their life while they might have still had further enjoyment in anticipation of a time when they will not.
Ultimately, their choice becomes an impossible one. ... To either live on whilst the circumstances of their existence are intolerable, or to end their life while they might have still had further enjoyment in anticipation of a time when they will not.
This was an impossible choice faced by Lecretia Seales by the time of her hearing in May this year. By that time she was paralysed on her left-side, was visually impaired, and was suffering from a number of debilitating side-effects of her treatment.[9] Furthermore, her prognosis for palliative care was bleak, being unlikely to be unable to avoid pain whilst remaining lucid.[10]
When Ms Seales sought a declaration that a physician’s administering their patient aid in dying is not murder or manslaughter and, furthermore, that it is not aiding or abetting a suicide for a physician to make the means of suicide available to their patient, she effectively sought to carve out a third choice for herself.[11] This third option would be to retain autonomy over the end of her life by being able to choose the moment when she died without having to ensure she retained the physical capacity to do so in a manner that would not imperil others around her when, and only when, her circumstances became intolerable.[12]
In pushing her case, therefore, Ms Seales argued that she was fighting to ensure she was not forced to endure “a death that is in no way consistent with the person that I am and the way that I have lived my life” by allowing her, as “a fiercely independent and active … intellectually engaged” person, to “have a voice in my death”[13] by retaining autonomy over the end of her life.
Justice Collins’ response to Ms Seales’ application begins with a brief survey of the wide range of cleavages in philosophical, moral, ethical, and clinical opinion that her application cut across; his Honour noting that Ms Seales’ application effectively sought to further curtail the law’s protection of the sanctity of human life on the grounds of individual autonomy. To do so, his Honour seemingly appreciates, would be to go beyond the principles in Airedale NHS Trust v Bland, as adopted here in Auckland Area Health Board v Attorney-General, that physicians cannot be obliged to treat a patient contrary to their wishes and are not required to treat a patient where it is best practice not do so, and to give full effect to Lord Keith’s dictum in Bland that the law should not “compel the temporary keeping alive of patients who are terminally ill where to do so would merely prolong their suffering”[14].[15]
His Honour notes that the argument in favour of preserving individual autonomy and dignity in these cases stands opposed to the need to protect the vulnerable.[16] Whilst, in this case, his Honour appears persuaded that Ms Seales’ application was being pursued “in a positive, rational, manner without showing any signs of depression or lack of full appreciation of her circumstances”[17], his Honour also notes that assessing if a patient is truly vulnerable is impossible.[18] Such vulnerabilities, his Honour accepts, may well result in patients rendered more vulnerable because of their learning difficulties, age, isolation, lack of mobility, the influence, interests, and authority of others, or lack of ability to communicate either feeling, or even being, pressured to seek out assisted suicide if it was made legal.[19]
The question of assisted suicide is therefore one, his Honour recognises, in which a balance needs to be struck between respecting the rights of the rational autonomous actor who wishes to avoid a painful death or incriminating those around them, and those whose lack of agency due to their individual or social circumstances may result in their being inevitability deprived of their right to life.[20]
These are both equal justice concerns; representing countervailing claims for the state to protect individual rights of equal value. It is therefore necessary to decide where best to strike some balance between these claims. Given the enormous potential for the violation of individual rights in either case, it is arguably impossible to make this choice with any degree of certainty.
Given the enormous potential for the violation of individual rights in either case, it is arguably impossible to make this choice with any degree of certainty.
As Justice Collins proceeds from considering the policy implications of his decision to the criminal law provisions, it becomes apparent that the Courts are not the appropriate place for that balancing exercise to take place. As has been noted in the context of judicial review, the adversarial adjective process practiced by the Courts is inapt to consider the polycentric policy considerations often engaged by decisions dealing with issues of political consequences, as the Courts cannot adequately capture the wide-ranging impacts of their decisions on the rights of citizens at large.[21] These limitations are equally apparent in cases such as Ms Seales’ case.
Furthermore, as Justice Collins was aware in handing down judgment in this matter, cases such as Ms Seales’ often require the Courts to address these concerns under urgency, so that the applicant may still be able to derive some benefit from a positive outcome of their application.[22] Arguably, it is therefore particularly unsatisfactory for the Courts to attempt to strike the impossibly fine balance warranted in this class of case, since they are therefore especially unlikely to have sufficient time to fully reason through their decision to a degree necessary to correctly balance the competing claims of the vulnerable and competent terminally ill individuals.
Further still, the Courts are unlikely to be willing to decide on these issues, as his Honour’s clear deference to the doctrine of parliamentary supremacy in this case makes clear. This is readily apparent in his treatment of ss 63 and 160(2)(a), in which his Honour quickly concludes that s 63 expresses a clear legislative intent to preclude the possibility of legally effective consent to the intentional infliction of death.[23] His Honour therefore rapidly establishes that, since any direct assistance in the suicide would therefore be done in the absent of consent, it would be at-least an assault, and would thus provide the requisite unlawful act for manslaughter contrary to s 160(2)(a).[24] In rejecting Ms Seales’ submission that s 63 is capable of being construed as precluding consent to death being a defence only where the infliction of death is contrary to public policy, which his Honour appears to accept it would not be in the case of an autonomous rational adult, his Honour therefore defers to Parliament’s clear statement that “the interest of the state in preserving human life overrides the otherwise all-powerful interest of patient autonomy”[25].
In doing so, his Honour respects Parliament’s having decided to weight the law in favour of protecting the lives of the vulnerable over the competing claims of autonomy and dignity, and declines to alter the balance of the law. This is particularly apparent in Justice Collins’ response to Ms Seales’ submission that s 179 was intended only to protect “those who feel that their lives are worthless or that they are a burden to others and therefore that they ought to end their lives even though they do not wish to do so”[26]; that is to say, that individual autonomy should prevail over the sanctity of life.[27]
In doing so, his Honour respects Parliament’s having decided to weight the law in favour of protecting the lives of the vulnerable over the competing claims of autonomy and dignity, and declines to alter the balance of the law.
In rejecting Ms Seales’ contention through a traditional exercise in statutory interpretation, his Honour makes two responses. The first is that s 179 was enacted alongside s 41, which empowers individuals to use reasonably necessary force to prevent suicides.[28] Noting that s 41 does not distinguish, as Ms Seales’ submission would require it to, between a rational suicide and suicides by vulnerable individuals, his Honour considered that for s 41 to have any effect it must apply to all suicides.[29] Accordingly, his Honour rejected Ms Seales’ attempting to define ‘suicide’ for the purposes of the Crimes Act 1961 in such a way as to distinguish between a suicide that is “irrational and a product of impaired thinking” and a “rational decision to die” my a mentally competent adult enduring a terminal illness.[30]
Whilst his Honour’s observation in regards to the effect of drawing such a distinction on the efficacy of s 41 is correct, it is, with respect, irreconcilable with his Honour’s broader dictum that there is “an important distinction between those who end their lives by taking a lethal drug and those who decline medical services and die from natural causes”[31], which latter category of persons his Honour would not regard as as committing suicide for the purposes of the Crimes Act. His Honour bases this distinction on the fact that, in the former case, the immediate cause of death is the lethal drug, whereas, in the latter case, it is the natural causes that eventuate from the decision to refuse medical services.[32] With respect to his Honour, that distinction ignores that, in both cases, the personal intentionally acts to end their own life, and the end of their life results from that voluntary decision.
Certainly, his Honour’s distinguishing between those who voluntarily end their own lives, those who take their lives for altruistic purposes, and those who are coerced into taking their own lives is correct, with only members of the first category really able to be called ‘suicides’ on the ordinary and natural meaning of the word.[33] That distinction, however, is also capable of being drawn in a manner favourable to Ms Seales’ claim. If s 179 is regarded as having been enacted only to protect the vulnerable from being pressured into committing suicide, then it might be regarded as seeking only to protect those in the third category above, since any person pressured into suicide is covered into end their own life. This would mean that the marginal note describing s 179 as prohibiting the “aiding or abetting suicide” is a misnomer, since it is not directed at those who voluntarily end their own life as a rational actor as they have not been coerced into ending their own life. On this reading, Parliament never intended to prevent a rational and autonomous actor from ending their own life.
That argument is not inconsistent with Justice Collins’ second response that ss 41 and 179 were enacted as part of the legislative complex that achieved the decriminalisation of attempted suicide in 1961.[34] Drawing from the parliamentary record giving this context, his Honour concluded that Parliament’s intent was a humanitarian one of protecting the vulnerable whilst removing the stigma of criminality from attempted suicide.[35] It was not intended to create a right to suicide; his Honour finding that such a legislative intention would be plainly incompatible with the law’s introducing a considerable penalty for assisting, abetting, counselling, or procuring a suicide.[36] If, however, the character of suicides is such that they are only the voluntary acts of rational individuals, rather than those coerced into ending their own life, as his Honour’s distinction would indicate, then that penalty is in fact imposed only on those who coerce others to end their own life at a moment of vulnerability.
Arguably, therefore, the distinction pressed for by Ms Seales identifies a means within the current framework of the law whereby an appropriate balance might be struck between the autonomy of the rational individual sufferer and the need to protect the vulnerable. Whilst, arguably, the current position is in fact compatible with the stated intention of Parliament in enacting ss 41 and 179, it is understandable, given the language of the statute, that Justice Collins felt unable to grant Ms Seales the declaration she sought in regards to her physician giving her the means to end her own life. Certainly, given the very clear language of s 63, it was very likely the Courts would find it impossible to address the proper balance of the competing claims in regards to her physician directly ending Ms Seales’ life.
Arguably, therefore, the distinction pressed for by Ms Seales identifies a means within the current framework of the law whereby an appropriate balance might be struck between the autonomy of the rational individual sufferer and the need to protect the vulnerable.
As his Honour noted in concluding his judgment, whilst Lecretia Seales did not drive the law in her desired direction, her case served to focus public attention on the numerous issues associated with the assisted suicide cases that have come before the Courts in recent years.[37] In doing so, hopefully, she has contributed to the emergence of a popular discussion about the two competing claims to protection of individual rights by the law raised by this case. Whilst, for the purposes of this analysis, one of these groups - those at risk of being pressured into suicide by the malicious animus of others or their distressing social circumstances - has been described as ‘vulnerable’, the other group is no less vulnerable. It is inequitable that sufferers of a terminal illness who do not wish to implicate their loved ones must often die alone before they have lived out the whole part of their life where their condition is not intolerable.
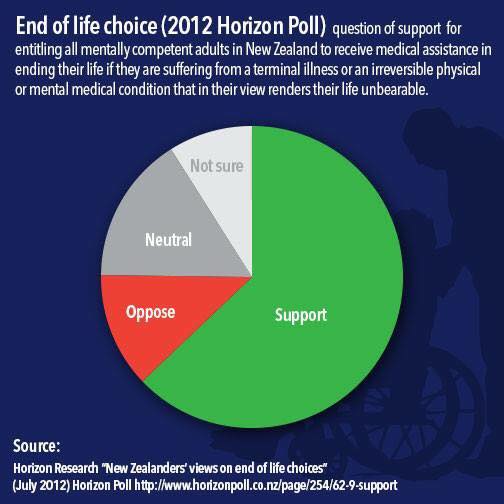
As Justice Collins notes, the balancing of these impossibly finely balanced claims to individual rights is best reserved for the legislature. As his Honour has noted, Parliament has demurred from discussing this potentially fractious issue in recent years. However, a recent article on this website presented evidence that over half of voters support granting a right “to all mentally competent adults in New Zealand to receive medical assistance in ending their life they are suffering from a terminal illness or an irreversible physical or mental condition that in their view renders their life unbearable.”[38]
In fact, this morning, the Prime Minister has been reported as saying that he "would probably support a euthanasia law change of the type Lecretia Seales wanted", and stated his view that " it was inevitable the topic would re-emerge in Parliament" as it had re-ignited public debate.[39] Critically, however, the Prime Minister said that he would leave the matter to arise through the private member bills process; meaning it may well be months or years until the issue is raised again.
The time for that discussion about the proper balancing of these claims is near, even if it has not quite yet arrived. It seems that it is very nearly time for the people of New Zealand to make a difficult choice; one that may potentially mean that those who find themselves in Ms Seales’ position in the future do not face an impossible choice.
I wish to express my condolences to the family, friends, colleagues, and loved ones of Ms Seales, who passed away last Friday morning the 5th of June of natural causes. May she rest in peace.
Where to get help:• Lifeline: 0800 543 354 (available 24/7)• Suicide Crisis Helpline: 0508 828 865 (0508 TAUTOKO) (available 24/7)• Youth services: (06) 3555 906• Youthline: 0800 376 633• Kidsline: 0800 543 754 (4pm to 6pm weekdays)• Whatsup: 0800 942 8787 (1pm to 11pm)• The Word Depression helpline: 0800 111 757 (available 24/7)• Rainbow Youth: (09) 376 4155• CASPER Suicide Prevention
---
[1] Crimes Act 1961, s 63.[2] Section 20.[3] Section 167(a).[4] Section 179(b).[5] Section 66(1)(c).[6] Seales v Attorney-General [2015] NZHC 1239 at [5] per Collins J.[7] At [29].[8] At [49]-[54].[9] At [25]-[26].[10] At [32]-[48].[11] At [5]-[7].[12] At [49].[13] At [29].[14] Airedale NHS Trust v Bland [1993] AC 789 (HL) at 859.[15] Auckland Area Health Board v Attorney-General [1993] 1 NZLR 235 (HC).[16] Seales v Attorney-General, above n 6, at [80].[17] At [81].[18] At [78].[19] At [77]-[79].[20] See New Zealand Bill of Rights Act 1990, s 9 for the affirmation of that right in New Zealand.[21] See Council of Civil Service Unions v Minister for the Civil Service [1985] AC 374 (HL); Burt v Governor-General [1992] 3 NZLR 672 (CA) for discussion of the limits of judicial review.[22] Seales v Attorney-General, above n 6, at [17].[23] At [89].[24] At [107]-[113].[25] Airedale NHS Trust, above no 14, at 893 per Lord Mustill.[26] R (Nicklinson) v Ministry of Justice [2014] UKSC 38 at [78] per Baroness Hale.[27] Seales v Attorney-General, above n 6, at [127].[28] At [120].[29] At [128].[30] At [135].[31] At [143].[32] At [144].[33] At [143].[34] At [129].[35] At [130]-[131].[36] At [131]-[132].[37] At [211].[38] Horizon Research “New Zealanders’ Views on End of Life Choices” (July 2012)[39] NZME “Key supports euthanasia, says it will be debated again soon” The New Zealand Herald (online ed, Auckland, 8 June 2011).
The views expressed in the posts and comments of this blog do not necessarily reflect those of the Equal Justice Project. They should be understood as the personal opinions of the author. No information on this blog will be understood as official. The Equal Justice Project makes no representations as to the accuracy or completeness of any information on this site or found by following any link on this site. The Equal Justice Project will not be liable for any errors or omissions in this information nor for the availability of this information.